
Page 51 - Virtual Vascular Vol 4
P. 51
In view of end-organ mal-perfusion (left kidney), deranged renal
function and difficult to control hypertension, he was treated by
thoracic endovascular aortic repair (TEVAR) with intentional coverage
of left subclavian artery origin to achieve an adequate proximal landing
zone, aiming to cover the entry intimal tear distal to left subclavian
artery and redirect blood to true lumen. Intravascular ultrasound and
intraoperative angiogram were used to ensure placement of guidewire
along the true lumen. Left vertebral artery was hypoplastic and left
common carotid artery to left subclavian artery bypass graft was
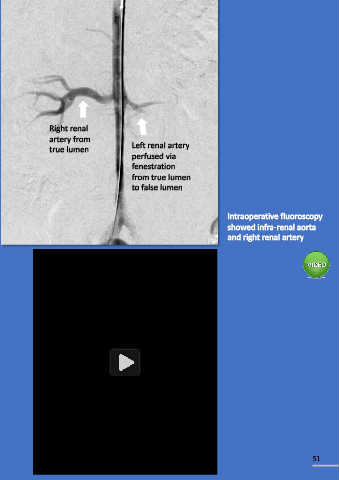
deemed unnecessary. As left renal artery was perfused from the false Right renal
lumen, left renal artery stenting was done through fenestration from artery from
the true lumen. Finally, left subclavian artery embolization was done to true lumen Left renal artery
perfused via
prevent Type II endoleak. fenestration
from true lumen
to false lumen
Intraoperative fluoroscopy
showed infra-renal aorta
and right renal artery
Cook Dissection
Animation.mp4
Diss2.mp4
50 51