
Page 30 - Virtual Vascular Vol 19
P. 30
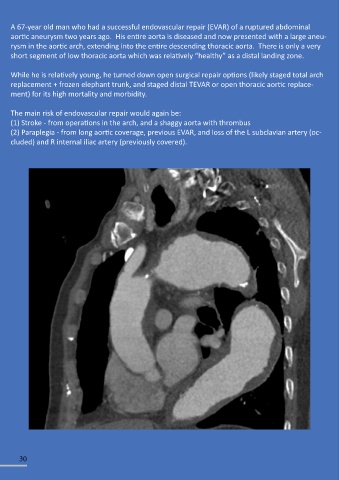
A 67-year old man who had a successful endovascular repair (EVAR) of a ruptured abdominal
aortic aneurysm two years ago. His entire aorta is diseased and now presented with a large aneu-
rysm in the aortic arch, extending into the entire descending thoracic aorta. There is only a very
short segment of low thoracic aorta which was relatively “healthy” as a distal landing zone.
While he is relatively young, he turned down open surgical repair options (likely staged total arch
replacement + frozen elephant trunk, and staged distal TEVAR or open thoracic aortic replace-
ment) for its high mortality and morbidity.
The main risk of endovascular repair would again be:
(1) Stroke - from operations in the arch, and a shaggy aorta with thrombus
(2) Paraplegia - from long aortic coverage, previous EVAR, and loss of the L subclavian artery (oc-
cluded) and R internal iliac artery (previously covered).
30