
Page 21 - Virtual Vascular Vol 8
P. 21
Aortic Anatomy
Retrograde Type A
intramural haematoma
The diagnosis was a Type B acute aortic dissection with intimal tear just distal to
left subclavian artery. However, it was complicated by a retrograde Type A
dissection to ascending aorta with a thrombosed false lumen, giving rise to a
intramural haematoma at the ascending aorta, turning this into a Type A
dissection.
The patient was operated on by cardio-thoracic surgeons. A total aortic arch
replacement under cardiopulmonary bypass was performed. Type A dissection
had a higher risk of fatal complications, such as coronary involvement, rupture,
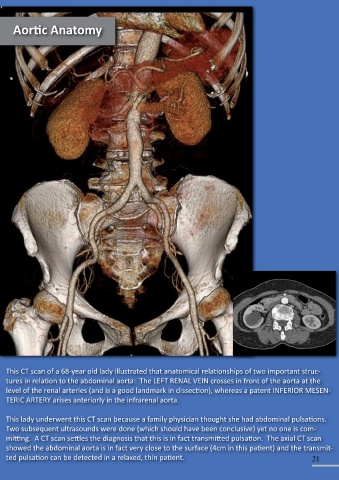
and cardiac tamponade. Emergency surgery is justified to reduce acute mortality This CT scan of a 68-year old lady illustrated that anatomical relationships of two important struc-
rates. tures in relation to the abdominal aorta: The LEFT RENAL VEIN crosses in front of the aorta at the
level of the renal arteries (and is a good landmark in dissection), whereas a patent INFERIOR MESEN-
TERIC ARTERY arises anteriorly in the infrarenal aorta.
This lady underwent this CT scan because a family physician thought she had abdominal pulsations.
Two subsequent ultrasounds were done (which should have been conclusive) yet no one is com-
mitting. A CT scan settles the diagnosis that this is in fact transmitted pulsation. The axial CT scan
showed the abdominal aorta is in fact very close to the surface (4cm in this patient) and the transmit-
20 ted pulsation can be detected in a relaxed, thin patient. 21